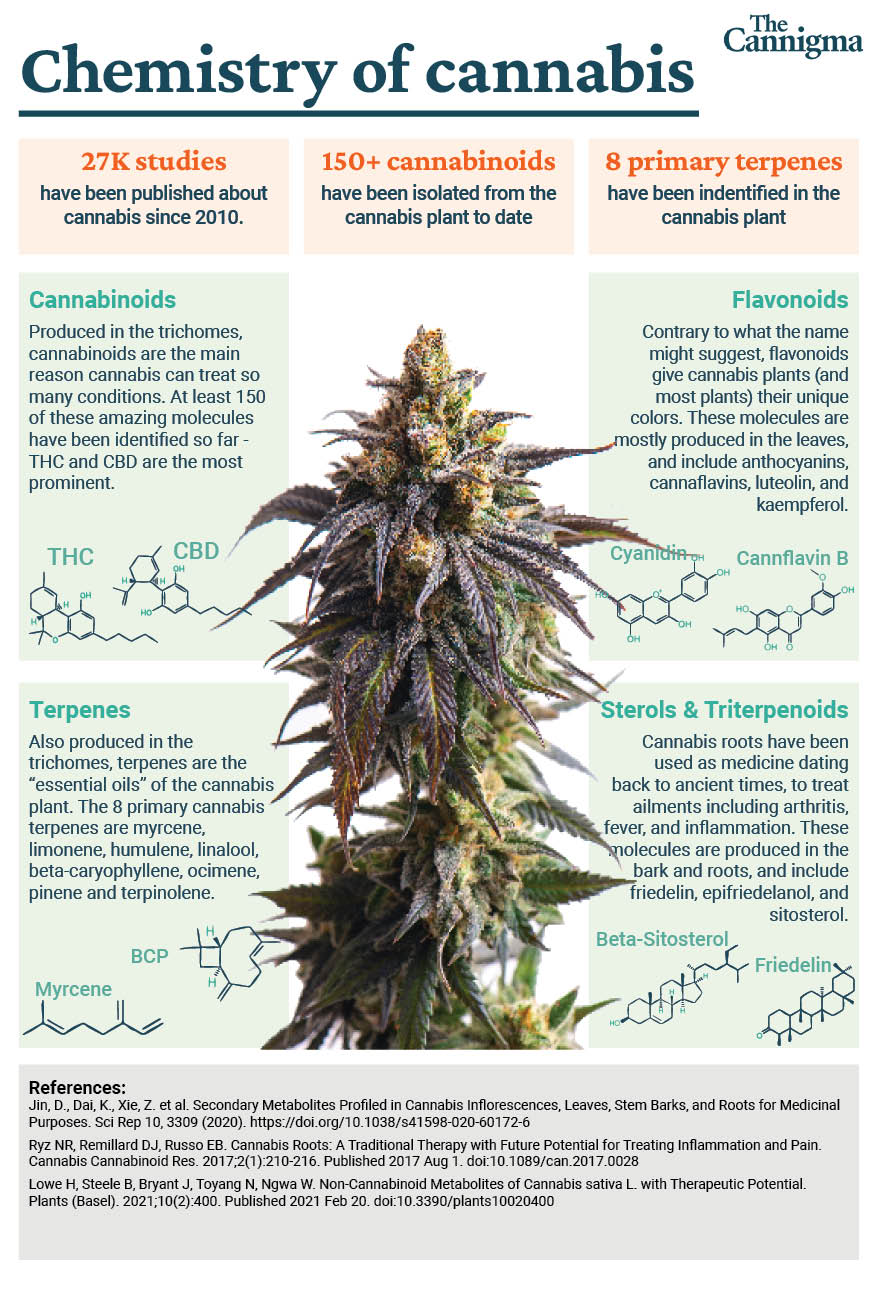
There are a lot of different molecules in nature, and though cannabinoids are rather rare, they are extremely abundant in cannabis (hence the name). THC is the most prevalent, famous and researched cannabinoid by far.
THC is the molecule responsible for the famous high associated with marijuana, but it also has a long list of therapeutic effects.

There are three main types of cannabis plants, all defined by their most abundant cannabinoids, and the most popular one is Type I, the THC dominant type. The other two types either have a balanced ratio of the non-intoxicating CBD and THC (Type II), or a high ratio of CBD with only trace amounts of THC (Type III).
What is THC?
THC is short for tetrahydrocannabinol. It is the molecule that is most associated with the cannabis plant, and for a good reason – it’s responsible for most of the effects created by cannabis, therapeutic or otherwise.
When talking about THC we usually refer specifically to delta-9 THC, but tetrahydrocannabinols are a family of cannabinoids that share a similar molecular structure.
Other members of the family that recently gained lots of attention in the United States are delta-8 THC (d-8) and delta-10 THC (d-10). Both are only found in trace amounts within the plant, but can easily be produced artificially in a lab.
The reason these two cannabinoids have become so popular in the United States is because of a legal contradiction created by the 2018 Farm Bill, which declared products derived from hemp to be legal. This contradiction, combined with a problematic regulatory framework that limits access to THC products in many states, has created a booming market for d-8 and d-10. The safety of using these products however, is still unknown.

Who discovered THC?
Raphael Mechoulam is often credited with discovering d-9 THC along with his colleague Yehiel Gaoni based on the study they published in 1963, when they isolated and identified the structure of delta-9 THC for the first time.1
However, the first researcher that identified and isolated THC was the American Roger Adams in the early 1940’s. The reason Mechoulam receives most of the credit for the “discovery” of THC is because he properly defined its molecular structure, making it more accessible for research and development, which is something Adams couldn’t do with the technology available at the time.2
THC vs CBD

In recent years, CBD (cannabidiol) started gaining popularity, eventually leading to the creation of an entire industry, with countless CBD infused products available, from oils, to bath bombs, dog treats and even infused fabrics.
Both THC and CBD are chemically very similar, but act extremely differently in the body. These two major cannabinoids are both considered psychoactive as they can affect your mind and mood, but unlike CBD, THC can also alter your consciousness, making it not only psychoactive but also intoxicating.
Other good examples of psychoactive drugs include caffeine (psychoactive but non-intoxicating) and alcohol (both psychoactive and intoxicating).
Additionally, THC and CBD have distinct therapeutic properties. For instance CBD is best known for its anti-anxiety, anti-inflammatory and anti-epileptic effects, while THC is most commonly used to help with nausea, pain and spasticity.
Here is a list of the potential effects of THC and CBD:3

| THC | CBD |
|---|---|
| Euphoria | Antipsychotic |
| Analgesic | Analgesic |
| Anti-inflammatory | Anti-inflammatory |
| Antiemetic | Anticonvulsant |
| Antioxidant | Antioxidant |
| Neuroprotective | Immunosuppressive |
| Antispasmodic | |
| Bronchodilator | |
| Antipruritic |
Is THC legal in the US?
As is often the case with cannabis, the question of legality can be confusing. There’s an FDA approved synthetic THC drug that is legal and accessible for the treatment of some types of nausea (Marinol), but it’s not popular, and there are often reports of side effects that are not typically seen with whole plant cannabis. Depending on the state you’re in, THC products may be legally accessible to any adult, and other states restrict access to medical patients only.
Marijuana (defined in the US as any cannabis plant where THC>0.3%) is a schedule I drug according to the DEA and FDA. Meaning that it has a high potential for abuse, it has no accepted medical treatment use and it’s not safe enough for use as a medicine.4
Despite advancements in research, evidence regarding the health effects of cannabis use remains elusive and there is no consensus within the medical community about which conditions it can treat.5
Many states that disagreed with the federal approach to cannabis started their own medical marijuana programs, and made it accessible for patients. This eventually led to the full legalization of cannabis in some states.
Outside of the US, different countries have their own approach to cannabis. In some countries marijuana is fully legal and accessible, and in others you can go to prison for possession of tiny amounts.

Why is marijuana illegal?

Cannabis has been used for medicinal, religious and recreational purposes for thousands of years, all around the world. For reasons that still remain unclear, the United States federal government waged a war on marijuana starting in the early 1930s, leading to the US prohibition and eventually to international prohibition in the early 1960s.
The key figure in leading the new US agenda against cannabis was Harry Anslinger, the first head of the Federal Bureau of Narcotics – a title now informally referred to as drug czar. It wasn’t enough for Anslinger to make cannabis illegal in the US, he also used his influence to include it in the UN’s convention on narcotic drugs, making it illegal internationally.
There are a number of theories explaining Anslinger’s motives, ranging from racism to political power to down right corruption and protectionism. Regardless of the true reason for cannabis prohibition, one thing is crystal clear- it was not based on science.
In fact, today’s scientific literature has endless evidence that cannabis is a much more effective drug than a lot of its popular alternatives, and it may also be safer.
In any case, one important thing to point out is that the regulatory status of cannabis in the United States has nothing to do with science. Rather, it was based on a policy that was created in the 1950s, before THC or CBD were isolated and before the endocannabinoid system was discovered.
Is THC safe?
Yes, cannabis is an extremely safe drug. In fact, there’s no one single recorded case of death following a cannabis overdose. It’s not even clear whether you can actually overdose from cannabis, or in the words of the World Health Organization:
“The toxicity of D-9 THC is very low compared to other recreational and pharmaceutical drugs…It has been calculated that a lethal dose in a 70 kg human would be approximately 4 grams, and that such a dose could not be realistically achieved in a human following oral consumption, smoking or vaporizing the substance”.
This isn’t to say that cannabis has no risks at all, but compared to other substances and medications, it can be considered very safe.
How to dose THC safely
Though THC is usually the most abundant active compound in cannabis, dosing THC and dosing cannabis isn’t the same at all. Here are some factors that can influence your experience:
- other cannabinoids and terpenes
- the consumption method you prefer
- your own unique biological makeup
Though it may be challenging, there is a way to approach dosing systematically and can make finding the right dose easier.
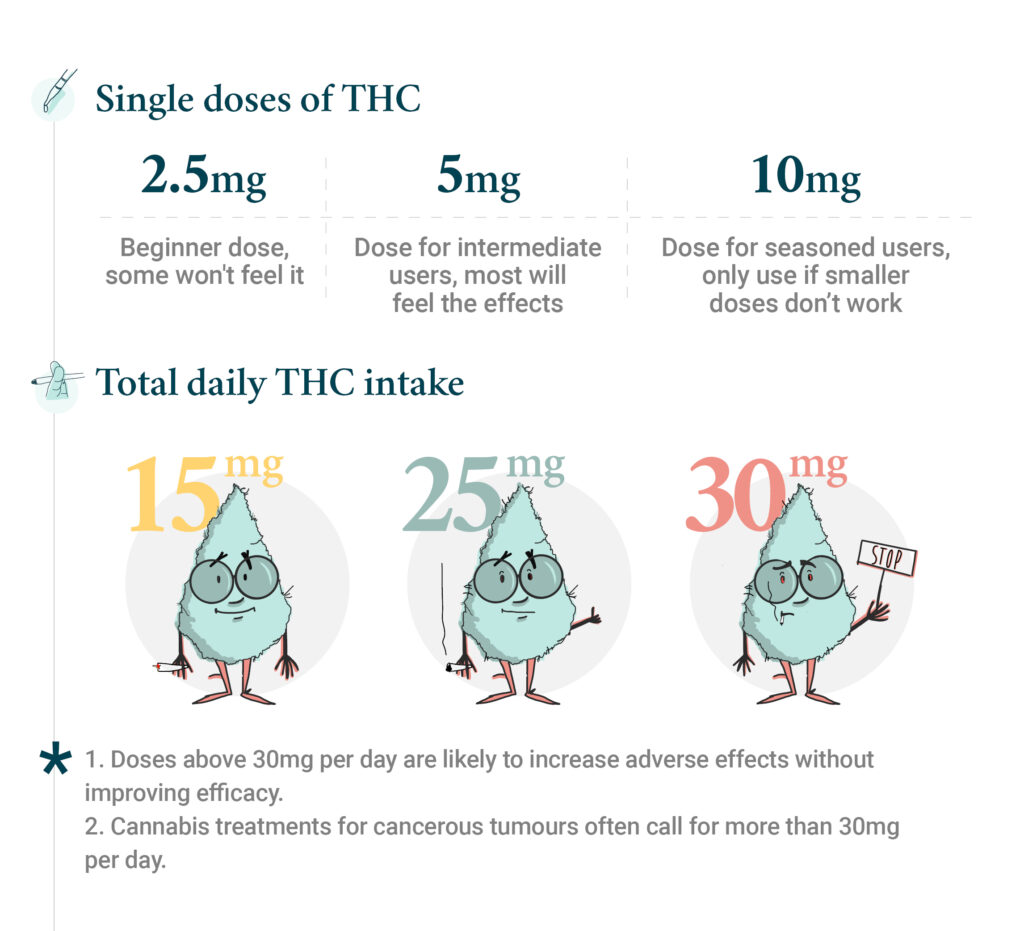
According to a review article co-authored by Dr. Ethan Russo, MD, broadly speaking, 2.5mg of THC is a good starting dose for inexperienced cannabis users. This should be enough to treat a variety of symptoms, but may go unnoticed for people with high tolerance to THC.
If you’re less sensitive to THC or if you’re an experienced user, 5mg of THC should be your ball park.
If you’re a very experienced user and these dosages don’t cut it, you can go as high as 10mg THC.
In terms of frequency, anything between 15-30 mg of THC daily is a good range. According to the existing research, higher dosages aren’t likely to be more efficient for treating symptoms, and there’s a much higher likelihood you’ll experience unwanted side effects.
One potential exception for these dosage guidelines is the treatment of cancerous tumors, where higher doses of THC are needed. But there’s very little research on that, and it’s mostly based on anecdotal evidence.
If you don’t have access to the THC concentration of your cannabis, the best approach in order to assess its potency would be to take one puff and wait for 15 minutes. Peak blood levels of THC usually occur in about 15 minutes, so it’s safe to assume that the effects won’t get much stronger after this timeframe.
This way, you’ll have a baseline to work with. If you feel a sufficient effect you can put your cannabis away, and if it’s not strong enough, you can take another puff. The same concept applies to ingested cannabis, only that here you’ll need to wait 2-3 hours in order to gauge the effects, because edibles take much longer to kick in.
Potential risks of THC
Being an extremely safe drug doesn’t mean there are no risks associated with cannabis consumption. The two main issues associated with cannabis, aside from immediate side effects like dry mouth, dry eyes, or anxiety, are Cannabis Use Disorder, and Cannabis Hyperemesis Syndrome.
Cannabis Use Disorder (CUD)
Cannabis Use Disorder is defined as “the continued use of cannabis despite impairment in psychological, physical, or social functioning.” In other words, if someone keeps using cannabis even if it has negative consequences, they suffer from CUD.
CUD is not a common condition, and it’s estimated one out of 10 cannabis users may suffer from it at some point during their relationship with cannabis. This is similar to the rate of excessive drinkers that suffer from alcohol dependence.
If you have a family history of addiction, or suffer from mental conditions such as depression and schizophrenia, you should carefully consider whether or not cannabis is right for you, particularly Type I cannabis.

Cannabinoid Hyperemesis Syndrome (CHS)
Mostly associated with heavy chronic users, Cannabinoid Hyperemesis Syndrome can cause nausea, vomiting, abdominal pain, weight loss, dehydration and a strong compulsion to take hot baths or showers. Usually all symptoms will decrease after 7-10 days of consuming cannabis.
It’s hard to assess the prevalence of CHS; it’s considered to be a rare condition, but reports vary from 0.003% of cannabis users, to as high as 35%.6
Other health concerns
Research suggests some marijauna users, particularly those who are already at risk, may be more likely to develop schizophrenia. This issue is controversial and the connection between cannabis use and psychotic illness is not well understood.7
There are concerns with consuming cannabis through inhalation, such as an increased risk of bronchitis, or swelling of the airways. However, this may be a result of smoking rather than THC itself.8
There was also a serious outbreak of EVALI associated with cannabis vaporizer pens, thought to be related to Vitamin E, but there aren’t thought to be any other serious safety concerns regarding cannabis e-cigarettes (ie vape pens). Studies are inconclusive about smoking cannabis use and cancer. It is evident in the research that smoking cannabis is not as harmful to the lungs and body as smoking cigarettes. Consuming marijauna or vaping THC is however correlated with smoking tobacco. While the risks of smoking cannabis have been difficult to measure, it is thought that the nicotine in tobacco smoke makes it much more harmful to the lungs than cannabis smoke. 9 10 11
THC and the entourage effect
There’s a widely held view among scientists that whole plants may serve as a better treatment than medication that uses only some active compounds in a plant. In the case of cannabis this would mostly relate to THC.
Though this view was never properly scientifically investigated, there’s an increasing amount of research that supports it. There are clinical studies that show pure cannabis is more efficient than cannabis-based pharmaceuticals, and that it may produce less adverse effects.
The “entourage effect” is a proposed hypothesis that explains exactly how cannabis as a plant may produce different effects than just isolated THC or CBD medications.
There are four proposed mechanisms for medicinal plants‘ synergistic effects, three of which are particularly relevant for cannabis. These include:
- Multi-target enhancing effects. On the one hand, one molecule can bind to many different receptors, and on the other many different plant molecules would bind to the same one receptor.
- Molecular movement enhancing effects. Plant molecules which are inactive by themselves (terpenes for example), may enhance the efficacy of active molecules such as THC and CBD.
- Modulation of adverse effects. Plant molecules that may reduce adverse effects. CBD for instance may modulate some of THC’s adverse effects.
Some researchers believe that the entourage effect can also explain why consuming different cannabis chemovars (also known as strains) may cause different experiences and effects.
That being said, there’s also some criticism on the entourage effects hypothesis, particularly regarding the enhancing effects, suggesting there’s not enough evidence to support it. But this may be as a result of lacking research studies.

Medicinal properties and benefits of THC
THC as a molecule has a long list of potential effects such as anti-inflammatory, antioxidant, neuroprotective and bronchodilator. While many of these effects are intriguing, due to significant barriers to research created through prohibition, most of what we know about it comes from preliminary research done on animals. Often these studies are conducted on animals such as mice, pigeons and monkeys, and the results don’t always translate directly to the human experience.
Given the complex nature of cannabis, where THC works differently in different doses and when accompanied by other cannabinoids and terpenes, it’s rather complicated to conduct clinical research. Consequently, the level of evidence for the different symptoms cannabis may treat varies, but most of the evidence is considered weak evidence by modern standards, which is one reason cannabis is not more widely accepted as having therapeutic effects.
Nevertheless, some of the most commonly accepted symptoms treated with cannabis high in THC include pain, nausea, and spasticity. Other conditions that may lack firm backing by clinical research, but are supported by growing anecdotal evidence, include insomnia, PTSD, convulsions, glaucoma, stress and anxiety (dose dependent), inflammatory bowel disease, insomnia and weight loss.
How does THC affect your mind and body?
Depending on the consumption method, the effects of THC may be felt within minutes (smoking/vaping) or a couple of hours (edibles).
The most common effects of THC (and cannabis in general), is a “high” or euphoria. But as mentioned, it may also help treat conditions such as pain, nausea and muscle stiffness.
How long does THC stay in your system?
These effects may last for four to seven hours in the case of inhalation, or up to 12 hours for edibles. But how long THC stays in your body and how long its effects last, are two different questions.
Your metabolism, body fat and gender may play a role in how long THC stays in your system. But other key factors that determine the window of detection are the testing method (blood, urine, hair, saliva, etc.) and the frequency and quantity of use.
THC can stay in your blood for 36 hours (single use) to 30 days (chronic use). Urine tests, however, may detect THC for 72 hours after a single use, and up to 90 days in chronic users.12
| Blood | Urine | Hair | Saliva | |
|---|---|---|---|---|
| Single use | 36 hrs | 72 hrs | Probably undetectable | 12 hours |
| Moderate use | 7 days | 14 days | 90 days | 2 days |
| Chronic use | 30 days | 30+ days | 90 days | 28 days |
| Notes | Detection window can vary highly depending on type of test cutoff level, metabolites screened, etc.13 14 | Detection beyond 30 days is uncommon but has been reported, especially in heavy use and in those with excessive body fat. 15 | The detection window is extremely long. The reason 90 days is the standard window testing facilities are looked at, but can vary from individual based on hair growth and based on laboratory procedures.16 | The smallest detection window of all testing types. Still, detection times vary depending on consumption method and test type. Smoking cannabis increases the likelihood of a positive saliva test due to mouth contamination.17 |
How THC affects your brain
THC interacts with the endocannabinoid system, which is particularly active in parts of the brain that manage your memory (hippocampus) and emotions (amygdala), and can also influence mood, sleep, and sensitivity to pain.
When you consume THC, depending on the dose, you may experience euphoria, anxiety, relaxation, disorientation, focus, confusion or changes in coordination.
This is closely related to a concept known as the biphasic effect, where smaller doses of THC can cause effects such as relaxation, anti-nausea and euphoria, while higher doses may cause opposite effects, like anxiety, paranoia and vomiting. Other factors that may play a role in your reaction to THC can include the type of product, other ingredients such as cannabinoids and terpenes, and your unique biology. Each person has a unique endocannabinoid system that is influenced by factors like genetics, diet, stress levels, and current cannabis use.

Adverse effects of THC
The most common mild side effects of THC include:
- red, dry, or itchy eyes
- dry mouth
- intense hunger (the munchies)
Other side effects include:
- impaired reaction time
- cognitive dysfunction
- short term memory loss
- drowsiness
More serious side effects that may occur include acute paranoia and/or anxiety that can last for a few hours, and in rare cases a few days.
THC products
One of the most important aspects to consider about cannabis products is quality. When it comes to production standards, marijuana products are much more regulated and supervised than CBD and hemp-derived products in general.
This has created a situation where marijuana products that are often treated as dangerous because they contain THC, are actually much safer and more accurately labeled than CBD products that lack regulatory oversight.
There are a number of ways to distinguish between THC products, but the main ones include the type of cannabis used (I, II or III), whether the product was infused with isolated THC or with an extraction of the entire plant (AKA full spectrum), the THC potency and the consumption method.
Isolated THC vs full spectrum THC
A lot of cannabis products are in fact regular products infused with a cannabis extraction. THC gummies for instance, are just regular gummies, to which THC isolate or cannabis extract was added during the production process.
Isolated THC
These are THC products that are based on isolated cannabis extract. The THC is extracted from the plant and the rest is discarded. This concentration of pure THC is then infused into the final product.
Products infused with isolated THC mostly include oils, edibles and topicals. In a sense, these products resemble THC pharmaceuticals as they only contain one active ingredient from cannabis.

Full spectrum
Some people prefer THC products that are more similar to the original plant. In full spectrum extraction, most of the active molecules in the plant are extracted, and then infused into the final product.
The difference between these two lines of products may resemble adding some rum to your cookies vs. mixing it with ethanol (pure alcohol). Rum would add flavors and aroma that ethanol doesn’t. It’ll probably feel different too. Sometimes the flavor and scent of cannabis can be very powerful in full spectrum products, which is why some people may prefer isolate-based products.
Broad spectrum
Between these two extremes there’s a middle way. Broad spectrum products contain numerous cannabinoids and terpenes, but have had the THC removed. Sometimes also called THC-free, broad spectrum may be desired by someone who can’t or doesn’t want to consume THC, but wants the rest of the extract to be representative of the plant. This is like adding virgin (alcohol-free) rum to your cookies. You’ll get the flavors of rum but without the kick of the ethanol.
Types of cannabis
The classification below mainly relates to cannabis flowers or joints, but can also be relevant for products infused with a full spectrum extraction. It has three main classes of cannabis chemotypes- I, II and III.
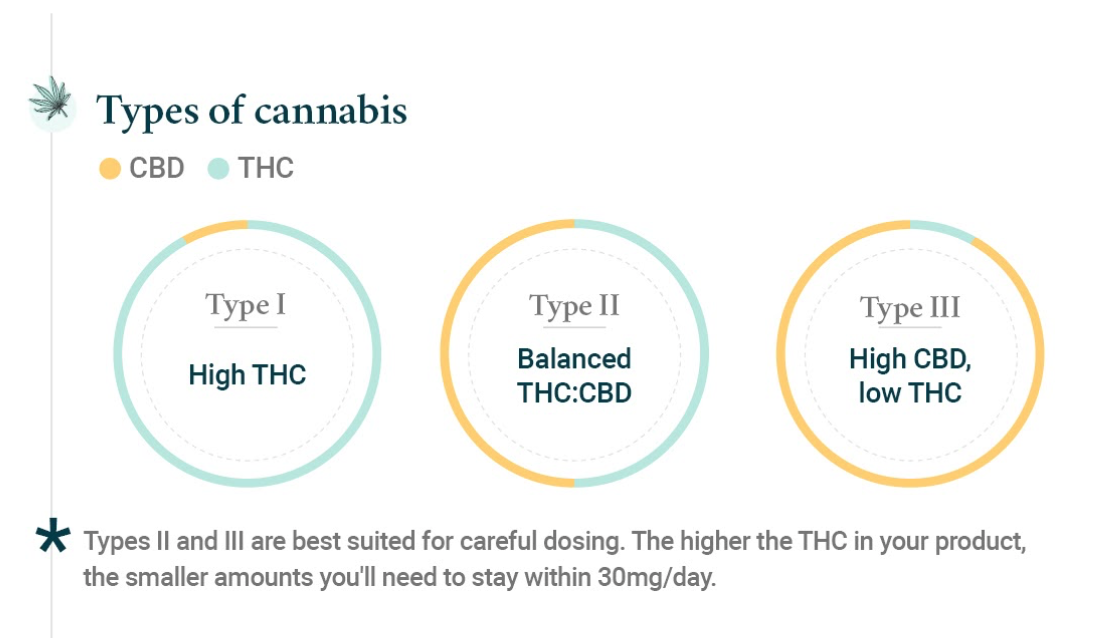
Type I cannabis: THC dominant plants
The dominance reflects on which active compounds are most abundant, rather than the potency of the product.
For example, a flower that contains 4% THC and 0.1% CBD would be classified as Type I, but so would a flower with 31% THC and 2% CBD.
Type II cannabis: Balanced THC:CBD ratio
Here there’s a more balanced amount of THC and CBD, but the same logic applies: it may be 1.3% THC and 1.8% CBD, but also 12% THC and 13%CBD. These products are still considered as marijuana products, and are often preferred when trying to avoid some of the main side effects of THC. The cannabis chemotype is a mainstay for medical use and is frequently a great place to start for new users.
Type III cannabis: CBD dominant cannabis
Though mostly perceived as CBD products, Type III cannabis sometimes contain considerable amounts of THC and can be mildly intoxicating. So technically speaking it can also be perceived as a THC product.
Type III can be recommended to new users, users that are particularly sensitive to THC, or those who are specifically looking for high concentrations of CBD.
Types of THC potency
Potency is one of the most important aspects to consider when deciding which cannabis products to use. In the past cannabis was completely illegal, so the average consumer couldn’t gauge the potency of their joint, because it couldn’t be tested in a lab.
Due to advances in breeding, cultivation, and plant science, the average cannabis flower has changed significantly over the past few years. Studies that analyzed samples of cannabis confiscated by the police, showed that the average joint had 3.4% THC in 1993, 8.8% in 2008, 12% in 2012 and 15% in 2018.18 19
That being said, within the regulated market, cannabis flowers with over 30% THC are not unheard of, and there are of course the endless list of cannabis concentrates that may have 60, 70 and even 80% THC.
Consumption methods
Another way to pick your THC product is based on consumption method. The main consumption methods are oral, inhalation, topical (dermal), and transdermal.
There are pros and cons for each method, though the scientific understanding about how they work varies a lot.
| Consumption method | Products | Pros | Cons |
|---|---|---|---|
| Inhalation | Vapes, joints, pipes, bongs, inhalers | Immediate symptom relief | Higher respiratory risks, shorter effects (1.5-2h) |
| Oral | Edibles, oils, anything you swallow. | Longer lasting effects, good as night treatment (6-12h), discreet | Slower onset (may take 1-2h to kick in), variable absorption makes it harder to dose and titrate |
| Oromucosal (sublingual) | Oils, tinctures, lozenges, tablets, powders, sprays, anything that can dissolve in the mouth. | Quick onset (15-45min), longer effect (6-8h), discrete | Variable absorption; some may be swallowed |
| Topical (dermal) | Creams, gels, balms, salves, (anything that goes on the skin and doesn’t isn’t going into the bloodstream.) | Local effects, quick onset | Lack of research, limited to local effects |
| Transdermal | Patches | Systematic effects, long lasting | Lack of research, difficult to dose and titrate |
Tetrahydrocannabinols
THC vs THCA
THCA is the original form of THC; this is how it’s produced in the cannabis plant. The plant makes THCA that is converted into THC during smoking. The main difference between the two cannabinoids, is that THCA won’t make you high, as it doesn’t interact with the CB1 receptors the same way.
Cannabis enthusiasts often refer to these as the “active” and “inactive” forms, but THCA is very much active. However, its mechanism of action is different and instead of getting you high will create other effects.
In order to transform THCA into THC it needs to be decarboxylated (heated). This can be done by putting it in an oven, or by smoking or vaping.
THCA research is still very limited and there’s much more we need to learn about it, but it has shown potential for the treatment of conditions such as obesity20, huntington’s disease21 and liver diseases.22
THC vs THCV
THCV is another rare cannabinoid with a similar structure to THC and although there’s limited research, it is known to cause a high.
This cannabinoid is usually found in small amounts in cannabis plants, but there are rare chemovars that produce higher amounts of THCV.
It has shown potential for a variety of conditions and symptoms such as obesity, diabetes, epilepsy, Parkinson’s disease, anxiety and osteoporosis.

D-9 THC vs D-8 THC
D-8 THC is a minor cannabinoid that appears in trace amounts in the cannabis plant, which can easily be produced semi-synthetically in a laboratory.
From a pharmacological perspective, it’s very similar to THC, and the very limited research that has been done on it suggests it has similar effects, just with lower potency. This is how D-8 THC products got the nickname “weed light”.
Recently D-8 THC products received a lot of attention because of a regulatory loophole that made them much more accessible than regular marijuana products. But despite lots of marketing efforts that suggest otherwise, D-8 THC is not federally legal and the DEA recently clarified that it is considered a Schedule I substance.
This is particularly important because there’s essentially no supervision on the manufacturers of these products. Meaning that unlike regulated products such as foods, beverages and pharmaceuticals, you can not trust the labeling of D-8 products. There’s no way to even tell if it’s actually D-8 or another substance, most commonly D-9 THC.
The main reason for the sudden hype around D-8 is to do with supply and demand. CBD manufacturers found themselves with lots of legal hemp, but not enough market. Since D-8 THC can be synthetically produced in a lab by using CBD, lots of CBD brands started marketing these products as well.
In general, if you live in a country with a regulated market, there’s no good reason to prefer D-8 THC over regular D-9 THC products. As opposed to hemp-derived products, the legal marijuana market is better regulated, more true to the plant, and much safer for consumers.
D-9 THC vs D-10 THC
This is an even newer trend in cannabis. D-10 also can’t really be found in the cannabis plant in any interesting quantities, but can be produced in a lab synthetically, again using CBD and chemically converting it.
Research on D-10 THC is almost non-existent, with only very few studies investigating its nature, none of which involves humans.
It’s highly advisable to avoid consuming D-10 THC products as there’s no knowledge about how they may affect humans, and much like D-8 THC, no supervision over production processes.
How does THC work?
THC and the endocannabinoid system
There are two main cannabinoid receptors, CB1 and CB2. They both play a major role in the activity of the endocannabinoid system (ECS), and they are both activated by THC.
Most of the therapeutic effects of cannabis and THC are mediated through their interaction with the ECS. These receptors are very abundant in the brain, particularly in areas relevant for conditions such as Parkinson’s disease, Alzheimer’s disease, autism spectrum disorder, epilepsy, stress and chronic pain.
But even in healthy people, the ECS is always active, and is crucial for memory and learning, appetite, sleep, pain perception, thermoregulation, immune system activity, and female reproductive process. This all may explain the different effects of THC/cannabis on the body.
To further complicate the matter, THC interacts with numerous receptors in the body which are not considered part of the classical definition of the ECS.
THC and GPR 55
This receptor interacts with so many cannabinoids that some researchers suggest it should be classified as CB3- a third ECS receptor. But for now, very little is known about how it works in general and how THC interacts with it in particular, so it’s not officially recognized as a part of the ECS. 23
One rodent study showed that mice that were genetically modified to not have GPR55 receptors, actually had a more enhanced sensitivity to THC. This suggests that GPR55 plays an important but different role than CB1 and CB2 as it relates to the effects of THC.24
Some of the conditions that GPR55 plays a role in are inflammatory and neuropathic pain and even as a potential therapeutic target in the treatment of cancer. 25 26
THC and 5-HT3A
The serotonin 3A receptors (5-HT3A) are intimately involved with the gut-brain connection. Activation of these receptors can lead to nausea and vomiting, which is why many pharmaceuticals used to treat nausea, like ondansetron, block 5-HT3A. Interestingly, THC is thought to also block this receptor and this action may be one of the many ways THC helps with chemotherapy induced nausea.27
THC and GPR18
The GPR 18 is another receptor that can be activated by THC. This receptor is not yet considered a part of the ECS, but like GRP55, it could be renamed one day in the future. Research suggests that THC may be able to reduce blood pressure by activating the GPR18 receptor.28 29
THC and PPAR-gamma
PPAR-gamma is a nuclear receptor involved in insulin sensitivity and glucose metabolism. It is well established that THC and other cannabinoids, including endocannabinoids 2-AG and anandamide, can activate PPAR-gamma and cause changes in cellular metabolism. THC may have actions at other PPAR receptors, but those findings have not yet been confirmed.
THC and TRPV2
TRPV2 is an ion channel, which is widely present in the nervous system and is involved in immune response, and may hold therapeutic potential in many conditions such as cancer30, epilepsy and diabetes. 31 32 33 34 35
CBD is a popular activator of TRPV2 receptors, but THC is considered to be the most potent cannabinoid on this target. The clinical significance of THC’s interaction with TRPV2 remains a focus of investigation.
Sources
- Gaoni Y. and Mechoulam R. (1964) Isolation, Structure, and Partial Synthesis of an Active Constituent of Hashish. Journal of the American Chemical Society 86 (8), 1646-1647 DOI: 10.1021/ja01062a046
- Adams R. Marihuana: Harvey Lecture, February 19, 1942. Bull N Y Acad Med. 1942;18(11):705-730.
- Russo, E. B., & Marcu, J. (2017). Cannabis Pharmacology: The Usual Suspects and a Few Promising Leads. Advances in pharmacology (San Diego, Calif.), 80, 67–134. https://doi.org/10.1016/bs.apha.2017.03.004
- https://www.dea.gov/sites/default/files/2020-06/Marijuana-Cannabis-2020.pdf
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Population Health and Public Health Practice; Committee on the Health Effects of Marijuana: An Evidence Review and Research Agenda. The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research. Washington (DC): National Academies Press (US); January 12, 2017.
- https://jim.bmj.com/content/68/8/1303
- Hasan A, von Keller R, Friemel CM, et al. Cannabis use and psychosis: a review of reviews. Eur Arch Psychiatry Clin Neurosci. 2020;270(4):403-412. doi:10.1007/s00406-019-01068-z
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Population Health and Public Health Practice; Committee on the Health Effects of Marijuana: An Evidence Review and Research Agenda. The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research. Washington (DC): National Academies Press (US); 2017 Jan 12. 7, Respiratory Disease. Available from: https://www.ncbi.nlm.nih.gov/books/NBK425753/
- Donald P. Tashkin & Michael D. Roth (2019) Pulmonary effects of inhaled cannabis smoke, The American Journal of Drug and Alcohol Abuse, 45:6, 596-609, DOI: 10.1080/00952990.2019.1627366
- Hindocha C, Shaban ND, Freeman TP, et al. Associations between cigarette smoking and cannabis dependence: a longitudinal study of young cannabis users in the United Kingdom. Drug Alcohol Depend. 2015;148:165-171. doi:10.1016/j.drugalcdep.2015.01.004
- Melamede, R. Cannabis and tobacco smoke are not equally carcinogenic. Harm Reduct J 2, 21 (2005). https://doi.org/10.1186/1477-7517-2-21
- Verstraete A. G. (2004). Detection times of drugs of abuse in blood, urine, and oral fluid. Therapeutic drug monitoring, 26(2), 200–205. https://doi.org/10.1097/00007691-200404000-00020
- Lee D, Huestis MA. Current knowledge on cannabinoids in oral fluid. Drug Test Anal. 2014;6(1-2):88-111. doi:10.1002/dta.1514
- Karschner EL, Swortwood MJ, Hirvonen J, et al. Extended plasma cannabinoid excretion in chronic frequent cannabis smokers during sustained abstinence and correlation with psychomotor performance. Drug Test Anal. 2016;8(7):682-689. doi:10.1002/dta.1825
- https://jim.bmj.com/content/68/8/1303
- Moeller KE, Kissack JC, Atayee RS, Lee KC. Clinical Interpretation of Urine Drug Tests: What Clinicians Need to Know About Urine Drug Screens. Mayo Clin Proc. 2017;92(5):774-796. doi:10.1016/j.mayocp.2016.12.007
- Hasan A, von Keller R, Friemel CM, et al. Cannabis use and psychosis: a review of reviews. Eur Arch Psychiatry Clin Neurosci. 2020;270(4):403-412. doi:10.1007/s00406-019-01068-z
- Mehmedic Z, Chandra S, Slade D, et al. Potency trends of Δ9-THC and other cannabinoids in confiscated cannabis preparations from 1993 to 2008. J Forensic Sci. 2010;55(5):1209-1217. doi:10.1111/j.1556-4029.2010.01441.x
- ElSohly MA, Chandra S, Radwan M, Majumdar CG, Church JC. A Comprehensive Review of Cannabis Potency in the United States in the Last Decade. Biol Psychiatry Cogn Neurosci Neuroimaging. 2021;6(6):603-606. doi:10.1016/j.bpsc.2020.12.016
- Palomares B, Ruiz-Pino F, Garrido-Rodriguez M, et al. Tetrahydrocannabinolic acid A (THCA-A) reduces adiposity and prevents metabolic disease caused by diet-induced obesity. Biochem Pharmacol. 2020;171:113693. doi:10.1016/j.bcp.2019.113693
- Nadal X, Del Río C, Casano S, et al. Tetrahydrocannabinolic acid is a potent PPARγ agonist with neuroprotective activity. Br J Pharmacol. 2017;174(23):4263-4276. doi:10.1111/bph.14019
- Carmona-Hidalgo B, González-Mariscal I, García-Martín A, et al. Δ9-Tetrahydrocannabinolic Acid markedly alleviates liver fibrosis and inflammation in mice. Phytomedicine. 2021;81:153426. doi:10.1016/j.phymed.2020.153426
- Overton HA, Babbs AJ, Doel SM, et al. Deorphanization of a G protein-coupled receptor for oleoylethanolamide and its use in the discovery of small-molecule hypophagic agents. Cell Metab. 2006;3(3):167-175. doi:10.1016/j.cmet.2006.02.004
- Wang XF, Galaj E, Bi GH, et al. Different receptor mechanisms underlying phytocannabinoid- versus synthetic cannabinoid-induced tetrad effects: Opposite roles of CB1 /CB2 versus GPR55 receptors. Br J Pharmacol. 2020;177(8):1865-1880. doi:10.1111/bph.14958
- Staton PC, Hatcher JP, Walker DJ, et al. The putative cannabinoid receptor GPR55 plays a role in mechanical hyperalgesia associated with inflammatory and neuropathic pain. Pain. 2008;139(1):225-236. doi:10.1016/j.pain.2008.04.006
- Andradas C., Caffarel M.M., Pérez-Gómez E., Guzmán M., Sánchez C. (2013) The Role of GPR55 in Cancer. In: Abood M., Sorensen R., Stella N. (eds) endoCANNABINOIDS. The Receptors, vol 24. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-4669-9_5
- Thompson AJ, Lummis SC. 5-HT3 receptors. Curr Pharm Des. 2006;12(28):3615-3630. doi:10.2174/138161206778522029
- Console-Bram L, Brailoiu E, Brailoiu GC, Sharir H, Abood ME. Activation of GPR18 by cannabinoid compounds: a tale of biased agonism. Br J Pharmacol. 2014;171(16):3908-3917. doi:10.1111/bph.12746
- Penumarti A, Abdel-Rahman AA. The novel endocannabinoid receptor GPR18 is expressed in the rostral ventrolateral medulla and exerts tonic restraining influence on blood pressure. J Pharmacol Exp Ther. 2014;349(1):29-38. doi:10.1124/jpet.113.209213
- Santoni G, Amantini C, Maggi F, et al. The TRPV2 cation channels: from urothelial cancer invasiveness to glioblastoma multiforme interactome signature. Lab Invest. 2020;100(2):186-198. doi:10.1038/s41374-019-0333-7
- Tyagi S, Gupta P, Saini AS, Kaushal C, Sharma S. The peroxisome proliferator-activated receptor: A family of nuclear receptors role in various diseases. J Adv Pharm Technol Res. 2011;2(4):236-240. doi:10.4103/2231-4040.90879
- O’Sullivan SE. An update on PPAR activation by cannabinoids. Br J Pharmacol. 2016;173(12):1899-1910. doi:10.1111/bph.13497
- Santoni G, Farfariello V, Liberati S, et al. The role of transient receptor potential vanilloid type-2 ion channels in innate and adaptive immune responses. Front Immunol. 2013;4:34. Published 2013 Feb 14. doi:10.3389/fimmu.2013.00034
- Maria Beatrice Morelli, Consuelo Amantini, Sonia Liberati, Matteo Santoni and Massimo Nabissi, “TRP Channels: New Potential Therapeutic Approaches in CNS Neuropathies”, CNS & Neurological Disorders – Drug Targets 2013; 12(2) . https://doi.org/10.2174/18715273113129990056
- Shibasaki, K. Physiological significance of TRPV2 as a mechanosensor, thermosensor and lipid sensor. J Physiol Sci 66, 359–365 (2016). https://doi.org/10.1007/s12576-016-0434-7



Sign up for bi-weekly updates, packed full of cannabis education, recipes, and tips. Your inbox will love it.