Merch
Merch Medical card
Medical card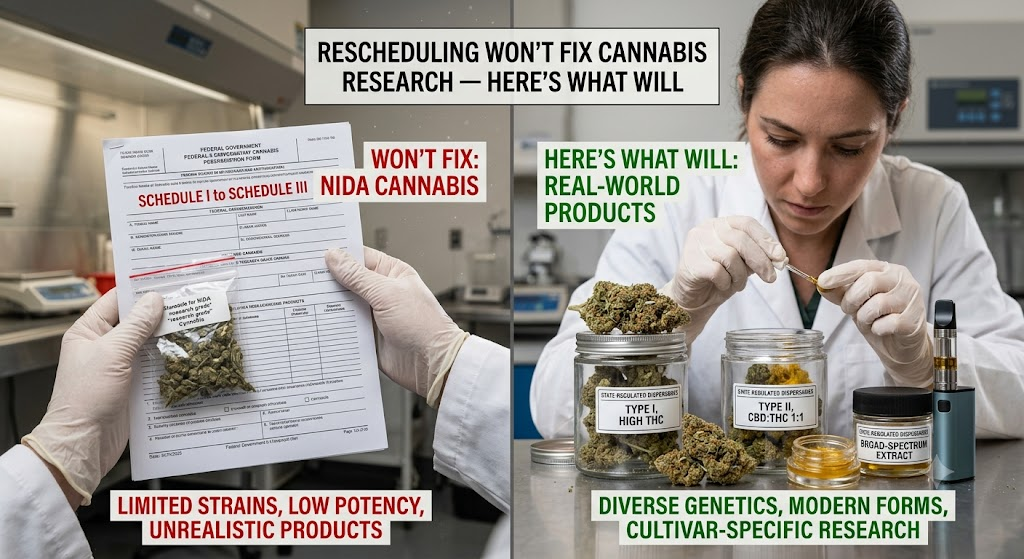
On June 29, the DEA begins a formal hearing to consider moving cannabis from Schedule I to Schedule III under the Controlled Substances Act. If it succeeds, it will be the most significant shift in federal cannabis policy in decades, and the headlines will be enormous.
But for the scientists, clinicians, and patients who have been waiting for rigorous, large-scale cannabis research to catch up with public use, Schedule III may feel like a long-awaited door opening onto another closed room.

Here’s the reality: rescheduling alone won’t fix the broken infrastructure that has hobbled cannabis research for 50 years. And understanding why matters, both for patients making health decisions today and for anyone following the longer arc of cannabis medicine.
What Schedule III Actually Changes
Rescheduling cannabis to Schedule III would have real and meaningful effects. It would remove the Section 280E tax burden for state-licensed medical operators, potentially reducing patient costs. It would ease some DEA registration requirements for researchers. And symbolically, it would signal that the federal government no longer classifies cannabis alongside heroin.1 2 3
For pharmaceutical companies developing FDA-approved cannabinoid medicines, Schedule III eases regulatory requirements while keeping federal oversight intact. That’s genuinely useful. The pipeline for cannabinoid-based pharmaceuticals, beyond Epidiolex, currently the only FDA-approved cannabis plant-derived drug, could see meaningful acceleration. 4 5
Schedule III removes some barriers. It doesn’t build the research infrastructure that was never built in the first place.
But the structural barriers that have made large-scale, rigorous clinical research on cannabis nearly impossible remain largely intact. Understanding them is essential.
The NIDA Monopoly Problem
For decades, researchers seeking to study cannabis in the United States have had to obtain it from a single federally licensed source: the University of Mississippi program operated under contract with the National Institute on Drug Abuse (NIDA). Since 1968, this arrangement created a notorious bottleneck: the cannabis available for research was often of poor quality, low potency, and limited variety compared to what patients and consumers actually use. 6 7
In 2021, the DEA began approving additional manufacturers to supply research-grade cannabis, which was a meaningful step. As of 2025, there are now seven DEA-approved bulk manufacturer cannabis growers, though NIDA paused new orders from Ole Miss following a DOGE-directed cost review, leaving the supply chain in some uncertainty. 8 9
Schedule III does not automatically resolve these supply challenges. The research supply chain problem requires separate regulatory action, dedicated funding, and institutional will.
The IND Barrier
Clinical trials involving cannabis in the US require an Investigational New Drug (IND) application with the FDA, a process designed for pharmaceutical compounds, not for a plant with hundreds of active constituents used in dozens of delivery methods. This creates a fundamental mismatch between the regulatory framework and the research question most patients and physicians actually have: does cannabis, as people use it, help with their condition? 10
Observational research and real-world evidence studies offer a workaround, but they carry less evidentiary weight than randomized controlled trials. The gap between what patients need to know and what the regulatory system allows researchers to rigorously study has not narrowed with rescheduling.
Funding Has Never Matched the Scale of Use
Cannabis is used by over 54 million Americans annually, making it one of the most commonly consumed psychoactive substances in the country. 11 Yet in 2021, NIH supported more than 785 cannabis research projects with total grant funding of $369 million, compared to $598 million for tobacco research and $568 million for alcohol research in the same year. Researchers responding to a 2022 NIH Request for Information identified increased funding as the single highest need in the field. 12 13 14
54 million Americans use cannabis annually. Federal research funding has never come close to matching that scale.
The Standardization Gap
One of the most persistent challenges in cannabis research is the absence of standardized products. When a clinical trial tests a specific dose of ibuprofen, every participant receives the same compound at the same dose. Cannabis research lacks this consistency: different cultivars, extraction methods, cannabinoid ratios, and delivery methods produce different effects in different patients.

This isn’t an unsolvable problem, but solving it requires investment in pharmaceutical-grade product development, standardization protocols, and validated delivery systems. Schedule III doesn’t fund or mandate any of that.
What Would Actually Move the Needle
If the research gap is the problem, the solutions are specific. Researchers and advocates have pointed to several concrete actions that would materially change what we know about cannabis medicine:
- Expanded federal licensing for research-grade cannabis suppliers, creating genuine competition and diversity in the research supply chain. 15 16
- Dedicated NIH funding streams for clinical cannabis research, matched to the scale of public use and health burden. 17 18
- Regulatory guidance from the FDA on observational and real-world evidence frameworks for cannabis that acknowledge it is not a single pharmaceutical compound. 19 20
- Congressional action on the SAFE Banking Act and related legislation that would allow cannabis-touching businesses, including research institutions, to access financial services without risk.
- International research partnerships, particularly with countries like Canada, Israel, and Germany where regulatory frameworks have permitted more robust clinical investigation.
The Patient’s Position
In the absence of the research patients deserve, millions of people are making decisions about cannabis for pain, anxiety, sleep, epilepsy, cancer symptom management, and dozens of other conditions based on incomplete evidence. They deserve better, not as a political statement but as a medical one.
Schedule III is a step. It is not a destination. The gap between what patients need to know and what science has been permitted to rigorously investigate has been building for fifty years. Closing it requires more than a scheduling change: it requires political will, dedicated funding, and a research infrastructure built from scratch.
The June 29 hearing matters. But the real work begins the morning after. 21 22
The Cannigma is an independent cannabis health and education platform. This article is for informational purposes only and does not constitute medical advice.
Sources
- DEA Federal Register Notice – Schedules of Controlled Substances: Rescheduling of Marijuana, April 28, 2026
- Foley Hoag LLP – DOJ Immediately Reschedules State-Licensed Medical Cannabis to Schedule III, April 24, 2026
- US Department of Justice – Justice Department Places FDA-Approved Marijuana Products in Schedule III, April 2026
- FDA – FDA Regulation of Cannabis and Cannabis-Derived Products, Including Cannabidiol (CBD)
- FDA – FDA and Cannabis: Research and Drug Approval Process
- NIDA – NIDA’s Role in Providing Cannabis for Research (Updated)
- NPR Health Shots – After 50 Years, U.S. Opens the Door to More Cannabis Crops for Scientists, May 2021
- The Marijuana Herald – NIDA Quietly Ends 57-Year Cannabis Supply Contract With University of Mississippi, July 2025
- Filter Magazine – NIDA Says It Halted Research-Cannabis Orders Due to DOGE Directive, July 2025
- FDA – FDA Regulation of Cannabis and Cannabis-Derived Products, Including Cannabidiol (CBD)
- Cannabis Promotions – US Cannabis Industry Statistics 2026: $33.8B market, 54.2M past-year consumers
- Journal of Cannabis Research – State Funding for Cannabis Research: An Analysis of Funding Mechanisms and Levels, March 2025
- NIH – NIH supported more than 785 cannabis research projects in 2021 with total grant funding of $369 million; compared to $598M for tobacco and $568M for alcohol research (same year)
- NIH – Researchers identified lack of sufficient research funding as the top barrier; 2022 RFI confirmed increased funding opportunities as highest need (2024 NIH report)
- NIDA – NIDA’s Role in Providing Cannabis for Research (Updated)
- NPR Health Shots – After 50 Years, U.S. Opens the Door to More Cannabis Crops for Scientists, May 2021
- Journal of Cannabis Research – State Funding for Cannabis Research: An Analysis of Funding Mechanisms and Levels, March 2025
- NIH NCCIH – Funding Opportunity for a Resource Center for Cannabis and Cannabinoid Research (RFA-AT-24-006)
- FDA – FDA Regulation of Cannabis and Cannabis-Derived Products, Including Cannabidiol (CBD)
- FDA – FDA and Cannabis: Research and Drug Approval Process
- NORML – NORML Seeks Seat at DEA Marijuana Rescheduling Hearing, May 2026
- Business of Cannabis – DEA on Shaky Legal Ground: Rescheduling under legal strain, June 1, 2026



Sign up for bi-weekly updates, packed full of cannabis education, recipes, and tips. Your inbox will love it.