Merch
Merch Medical card
Medical card


Within four months, the Trump administration signed two executive orders that together mark the most consequential shift in federal cannabis policy and drug scheduling in over 50 years. On December 18, 2025, an order directed the Attorney General to expedite cannabis rescheduling from Schedule I to Schedule III. Then, on April 18, 2026, a second order directed the FDA and DEA to establish a patient access pathway for psychedelic compounds, including ibogaine, under the Right to Try Act, and allocated $50 million for federal-state research collaboration.
The political logic connecting both orders is the same: veterans, mental health, and bipartisan pressure. The science behind them is not, and the gap between those two facts is the most important thing to understand about this moment.

What Cannabis Rescheduling and the Ibogaine Order Would Actually Do
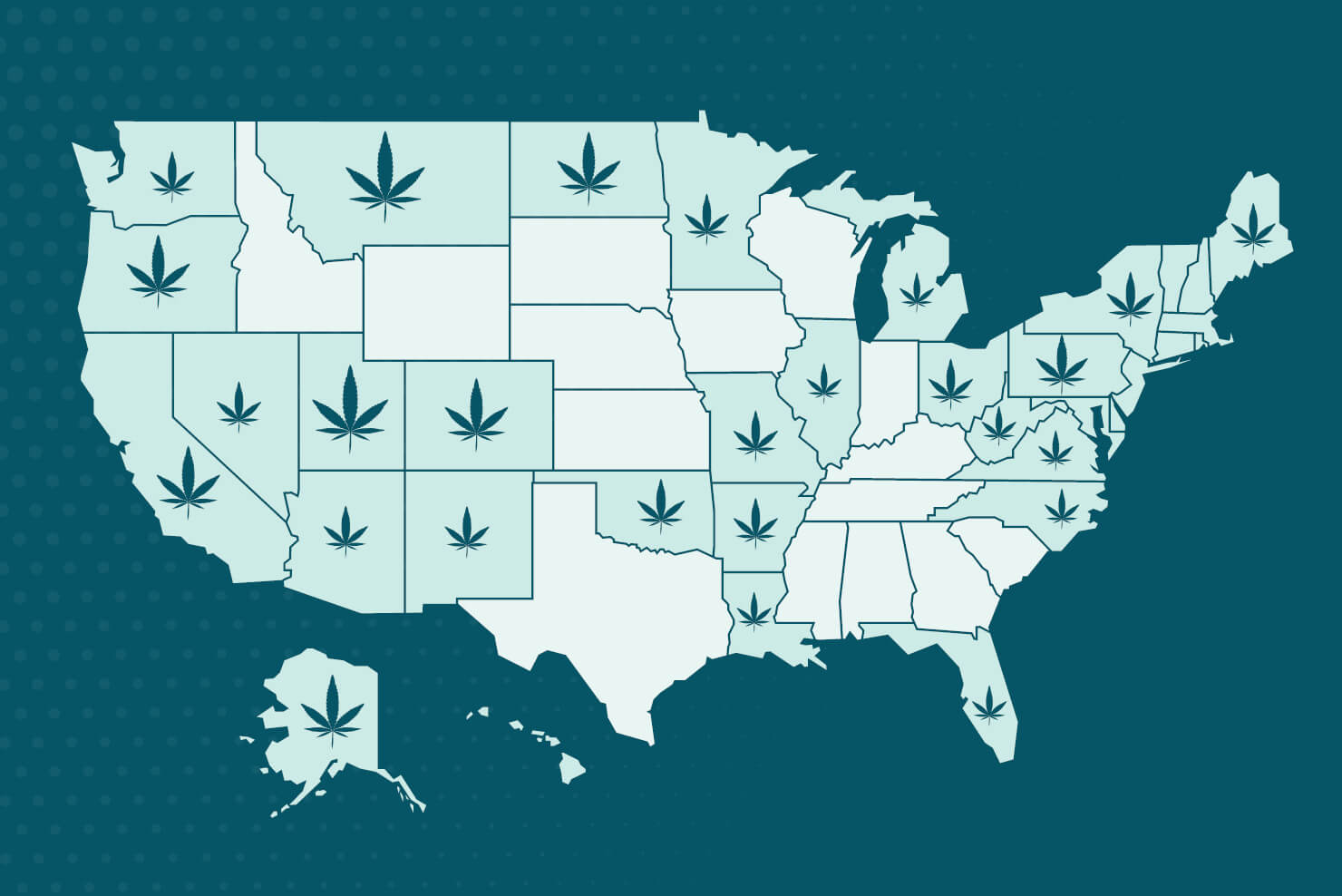
Neither order carries immediate force of law. Cannabis rescheduling remains proposed, not final. Scheduling hearings are still pending, and no final rescheduling action has occurred as of this writing. A February 2026 peer-reviewed analysis in Cannabis and Cannabinoid Research confirms that Schedule III status would deliver real changes: relief from the Section 280E tax burden that has choked state-licensed operators, modified criminal penalties, and expanded research access. Federal-state legal conflict would continue, since cannabis would remain a controlled substance under federal law. States have created their own regulatory frameworks under ongoing federal prohibition; Schedule III would not resolve that conflict.
The ibogaine order carries a different legal complication. Harvard Law’s Petrie-Flom Center flagged that ibogaine may not meet the eligibility requirements of the Right to Try Act, which requires completion of Phase I clinical trials. Ibogaine has not cleared that bar. The order is a strong political signal with real procedural uncertainty attached.
How Veterans Drove Cannabis Rescheduling and Ibogaine Reform
Veterans advocacy explains how ibogaine moved from clinical obscurity to presidential priority. Psychedelic therapy for veterans, long pursued outside U.S. borders, built the political case from the ground up. The organization VETS (Veterans Exploring Treatment Solutions) has helped secure more than $124 million in public funding for psychedelic research and has driven a series of landmark policy wins at the state and federal levels. U.S. veterans seeking relief from PTSD and traumatic brain injury have traveled to clinics in Mexico for ibogaine treatment, and their accounts — circulated through advocacy networks and congressional testimony — shifted the political calculus.
Texas Governor Greg Abbott signed Senate Bill 2308 in 2025, granting state matching funds for ibogaine research, with an explicit veterans rationale: Texas is home to more veterans than any other state. In March 2026, Utah passed legislation authorizing psychedelic-assisted therapy research for veterans with treatment-resistant PTSD. Utah has one of the largest per-capita veteran populations in the country and a veteran suicide rate more than double the national average.
This dynamic mirrors the political arc of medical cannabis. Patient advocates, many of them veterans, built the credibility that cracked open state legislatures in the 1990s and 2000s. A 2026 survey of state-level psychedelic reform activity shows activity in more than 10 states, including Oregon, New Mexico, Mississippi, and Alaska. Federal action is following state momentum, not leading it.
What the Ibogaine Evidence Actually Shows
The single most influential piece of evidence driving current ibogaine policy is the 2024 MISTIC study, published in Nature Medicine. The study enrolled 30 male Special Operations Forces veterans and reported large reductions in PTSD, depression, and anxiety one month after ibogaine treatment, with effect sizes (Cohen’s d of 2.54 for PTSD, 2.80 for depression) that are substantial by any clinical standard, and no unexpected serious adverse events.
The study’s limitations are equally important. It was open-label, uncontrolled, enrolled only male SOF veterans, and included no placebo comparison. Treatment took place in Mexico. The study cannot establish causation. A 2022 systematic review in the Journal of Substance Abuse Treatment found that available data suggest ibogaine has efficacy for opioid use disorder and cocaine use disorder, but the review emphasized the necessity of controlled clinical studies. No published randomized controlled trials exist for ibogaine. The evidence base consists of observational studies, open-label trials, case series, and preclinical data.
Cardiac Risk: The Safety Floor for Ibogaine Research
Ibogaine blocks the hERG potassium channel, causing QT interval prolongation and placing it in the same risk category as several approved medications with known cardiac profiles. A February 2026 scoping review in Molecules synthesized available safety data and confirmed that ibogaine has been associated with more than 30 deaths, according to MAPS, most occurring in unsupervised settings without cardiac monitoring. The Stanford MISTIC protocol used magnesium co-administration specifically to manage this risk. Medically supervised administration with cardiac monitoring is the minimum safety standard for any legitimate ibogaine research pathway — not an optional precaution.
Cannabis Rescheduling Rests on a Different Evidence Base
Cannabis and ibogaine operate through entirely different pharmacological mechanisms. Preclinical research shows that endocannabinoid system activity influences functional connectivity between the prefrontal cortex and amygdala, and that CB1 receptor activation within the amygdala may support extinction of fear memories, mechanisms particularly relevant to PTSD. The cannabis rescheduling order itself references that HHS found credible scientific support for cannabis use in treating pain, anorexia related to certain medical conditions, and chemotherapy-induced nausea.
Cannabis has a more mature evidence base than ibogaine, with decades of observational data and a growing clinical trial literature that has expanded alongside cannabis research access in states with regulated frameworks. The marijuana rescheduling debate has also surfaced that base’s limits. That base has its own weaknesses, particularly for psychiatric indications, where large randomized controlled trials are scarce and study designs vary considerably. A peer-reviewed analysis in Addiction confirms that evidence for cannabinoids in treating mental health disorders and substance use disorders is thinner than policy discourse implies. Both substances are advancing politically at a pace that outruns their clinical trial evidence.
A Warning from the Cannabis Playbook
The same Addiction analysis that mapped the cannabis-to-psychedelics policy parallel also issued an explicit caution: cannabis reform created a multibillion-dollar commercial ecosystem before the evidence base had matured. For-profit industry shaped regulatory frameworks in ways that served investment timelines over public health outcomes. Researchers and advocates working on ibogaine face the same risk if commercial incentives accelerate ahead of rigorous trial data.
A STAT News analysis published April 20, 2026, authored by practitioners with decades of addiction treatment experience, raised a related concern: the pharmacocentric framing of ibogaine, which emphasizes compounds, protocols, and neurological mechanisms, tends to minimize the social determinants of sustained recovery. Community, relationships, and recovery capital remain the strongest predictors of long-term outcomes. That was true for cannabis treatment frameworks too, and policy often failed to account for it.
There is also a supply chain dimension that federal funding frameworks have not addressed publicly. Ibogaine is derived from Tabernanthe iboga, a shrub native to Gabon that sits at the center of the Bwiti spiritual tradition. Sharply rising global demand has strained iboga stocks, with reports of poaching in national parks and illicit supply chains bypassing indigenous communities. Whether the $50 million in federal matching funds will engage this dimension, or assume pharmaceutical synthesis will route around the plant entirely, remains unanswered.
The political conditions that brought cannabis and ibogaine to the same federal moment in 2026 are genuine and worth understanding. The convergence is political, driven by veterans, bipartisan mental health concerns, and years of state-level momentum. For researchers, clinicians, and patients following both pathways, the more relevant question is whether the science and the regulatory infrastructure will keep pace with the politics, and whether the mistakes of the cannabis policy era will teach reformers anything at all.
Frequently Asked Questions
Does cannabis rescheduling to Schedule III mean federal legalization?
No. Rescheduling cannabis from Schedule I to Schedule III would change its regulatory classification, but cannabis would remain a controlled substance under federal law. The most concrete near-term changes would include relief from the Section 280E tax burden for state-licensed operators, expanded research access, and modified penalties. Federal-state legal conflict would continue.
What is ibogaine, and why is it part of a federal executive order?
Ibogaine is a psychoactive compound extracted from Tabernanthe iboga, a shrub native to Gabon and Central Africa. Researchers have studied it as a potential treatment for opioid use disorder and PTSD. Veterans advocacy groups, citing promising but preliminary clinical results, helped push ibogaine from clinical obscurity to a 2026 executive order directing the FDA and DEA to explore a Right to Try access pathway.

What did the MISTIC study find about ibogaine?
The 2024 MISTIC study enrolled 30 male Special Operations Forces veterans and reported large reductions in PTSD, depression, and anxiety one month after ibogaine treatment. Effect sizes were substantial by clinical standards. The study had significant limitations: it was open-label and uncontrolled, enrolled only male SOF veterans, and included no placebo comparison. It cannot establish causation.
Is ibogaine safe?
Ibogaine carries documented cardiac risks, including QT interval prolongation, which has been associated with more than 30 deaths, according to MAPS. Most deaths occurred in unsupervised settings. The Stanford MISTIC protocol used magnesium co-administration and cardiac monitoring to manage these risks. Ibogaine should only be administered with medical supervision and cardiac monitoring in place.
How is cannabis policy different from ibogaine policy right now?
Cannabis has decades of observational data, a substantial (though imperfect) clinical evidence base for pain and chemotherapy-related nausea, and an established commercial infrastructure across dozens of states. Ibogaine has highly promising but methodologically limited preliminary data, no completed randomized controlled trials, a documented cardiac risk profile, and no regulated commercial supply in the U.S. The two substances share a political moment in 2026, not an evidentiary footing.



Sign up for bi-weekly updates, packed full of cannabis education, recipes, and tips. Your inbox will love it.