Merch
Merch Medical card
Medical card

A pharmacology-grounded look at what THC does to the brain’s fear circuitry when you get too high on cannabis, why edibles hit so much harder, and what the evidence actually supports for getting through it.
Getting too high on cannabis produces a recognizable cluster of symptoms: racing heart, spiking anxiety, paranoia, and sometimes a dissociative feeling that the world has gone strange. These reactions are unpleasant, and they’re also pharmacologically predictable. Knowing what drives them, why edibles are especially prone to triggering cannabis overconsumption episodes, and what the evidence supports for getting through them gives you something more useful than panic.
Why the Same Cannabis That Relaxes You Can Make You Too High: The Biphasic Effect
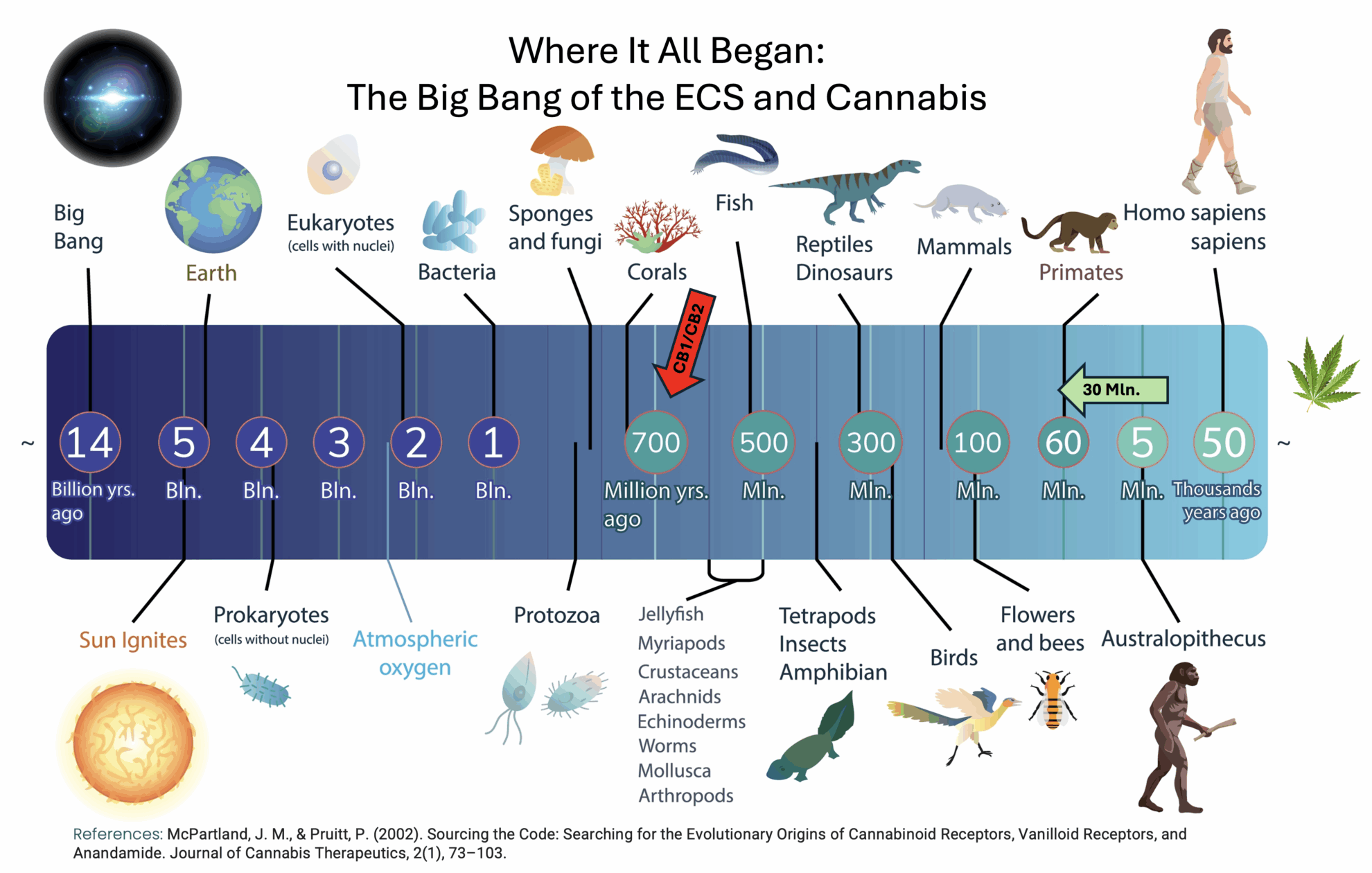
THC binds to CB1 receptors concentrated in the amygdala, hippocampus, and prefrontal cortex. At low to moderate doses, CB1 activation suppresses fear circuitry and produces the relaxation and euphoria cannabis is known for. At high doses, the mechanism flips. A 2017 human neuroimaging study found that THC-induced anxiety correlated with CB1 receptor availability in the amygdala, establishing a direct neural basis for why the same compound that calms one person can produce fear in another, and why the same person can have opposite experiences depending on dose.

A systematic review covering animal and human studies on cannabinoids and anxiety confirmed the biphasic dose-response across multiple experimental models: anxiolytic at low doses, anxiogenic at high doses. The receptor mechanism is consistent. The dose threshold at which this flip occurs varies between individuals, and that variability is part of why overconsumption episodes feel unpredictable even to experienced consumers.
Why Edibles Hit So Much Harder, and the Redosing Trap That Makes It Worse
Edibles don’t hit harder simply because people eat too many. The pharmacokinetics are different. After oral ingestion, the liver converts delta-9-THC into 11-hydroxy-THC (11-OH-THC) through first-pass metabolism via CYP2C9 and CYP3A4 enzymes. According to a 2024 clinical pharmacology review in The Permanente Journal, the ratio of 11-OH-THC to delta-9-THC exceeds 1:1 after oral ingestion, compared to less than 1:20 after inhalation. This metabolite crosses the blood-brain barrier more efficiently and produces stronger, longer-lasting intoxication. Most people who report getting too high from weed for the first time describe an edible, not a joint.
The onset delay of 30 minutes to two hours creates the classic redosing trap. By the time the second dose registers, the first is still peaking. The more potent 11-OH-THC metabolite can produce psychogenic effects, including acute distress, in people who redose because the initial effects haven’t appeared. Oral bioavailability for edibles also runs considerably lower and more variable (4–20%) than inhalation (30–60%), which means a dose that feels moderate when smoked cannot be assumed to translate proportionally when eaten.
What Being Too High on Cannabis Actually Feels Like
“Too high” covers several distinct experiences worth separating. Panic and anxiety are the most common, occurring with sudden onset during or shortly after inhalation, or more gradually 1–2 hours after an oral dose. Paranoia involves heightened threat perception with intact awareness that the perception may be distorted. Depersonalization (watching yourself from outside) and derealization (the sense that surroundings aren’t quite real) are common and can be alarming, but they differ from psychosis in one specific way: reality testing stays intact throughout.
A large observational study of 1,135 patients evaluated for acute cannabis toxicity in the emergency department found that 17.3% presented with cannabis-induced anxiety disorder. Among those patients, panic attacks occurred in 11.7%, and hallucinations in 6.1%. Edible cannabis use, younger age, and psychiatric comorbidities all increased risk in that cohort.
Who Is More Likely to Get Too High, and Why
Risk factors for a dysphoric cannabis experience include infrequent use, high doses, high-THC/low-CBD products, a personal history of anxiety disorders, elevated baseline anxiety at the time of use, and female sex. A 2023 review in the International Journal of Molecular Sciences found that genetic polymorphisms in CNR1 (the CB1 receptor gene) and FAAH (which regulates endocannabinoid breakdown) contribute to meaningful individual variability in response to the same dose of THC. Prior cannabis tolerance reduces but does not eliminate the risk, particularly with high-potency contemporary products.
The University of Washington’s Alcohol and Drug Abuse Institute literature synthesis on cannabis and anxiety disorders identifies a consistent theme across multiple lines of evidence: vulnerability is not randomly distributed, and individual response to THC is shaped by factors a person can often identify in advance.
The Potency Context Matters
A peer-reviewed analysis of DEA-confiscated cannabis samples documented THC concentration rising from approximately 4% in 1995 to approximately 12% in 2014, while CBD content fell from approximately 0.28% to less than 0.15%, shifting the THC-to-CBD ratio from roughly 14:1 to 80:1. Dispensary concentrates now routinely exceed 70–90% THC. Dosing intuitions built on older cannabis do not transfer to contemporary high-potency formats, and harm-reduction guidance written for earlier decades assumed a different product.
What to Do When You’re Too High: What the Evidence Actually Supports
Evidence-Based Ways to Come Down from Being Too High
Time is the primary evidence-backed intervention. Acute cannabis toxicity follows a self-limiting course, and the clinical standard is supportive care: a calm, quiet environment, reassurance that the experience will pass, rest, and hydration. A systematic review of pharmacological treatments for acute cannabis intoxication found benzodiazepines appropriate for severe agitation and antipsychotics for transient psychosis in clinical settings. For non-emergency episodes, the approach is the same minus the medication.
Grounding techniques, such as the 5-4-3-2-1 sensory method (naming five things you can see, four you can feel, three you can hear), carry solid evidence for general acute anxiety reduction. Their application to cannabis-induced panic has not been studied in controlled trials, but the extrapolation is reasonable and low-risk. Controlled breathing (slow exhale, longer than inhale) activates parasympathetic tone and may help reduce the subjective sense of physical threat.
CBD’s capacity to modulate THC-induced anxiety at the receptor level has some support. A 2023 systematic review of THC, CBD, and anxiety found evidence that CBD provided relief when baseline anxiety was low and partial relief when it was moderate, though this finding comes from laboratory THC-challenge designs rather than naturalistic overconsumption. Real-world evidence for CBD as an after-the-fact rescue intervention is thin.
Black pepper contains beta-caryophyllene (BCP), a sesquiterpene that a foundational 2008 PNAS paper established as a selective CB2 receptor agonist and functional dietary cannabinoid. CB2 receptors are concentrated in peripheral and immune tissues, not in the central fear circuits where THC-induced anxiety originates. The folk remedy has plausible chemistry and no human trial data. Sniffing or chewing black pepper causes no harm and may provide a grounding sensory anchor, but consumers should treat it as comfort, not antidote.
When to Seek Medical Care After Cannabis Overconsumption
Seek medical attention if you experience chest pain, loss of consciousness, prolonged vomiting, extreme confusion that does not resolve, or any symptom that genuinely frightens you. First-time or pediatric exposures should always be assessed. Cannabinoid hyperemesis syndrome (CHS), associated with chronic heavy use, requires clinical evaluation. For most adults in an uncomfortable but uncomplicated overconsumption episode, a calm space, water, and time remain the appropriate response.
Frequently Asked Questions
What does being too high on cannabis feel like?
A cannabis overconsumption episode typically involves some combination of racing heart, spiking anxiety, paranoia, and a dissociative sense that surroundings have become unreal. These experiences vary by person and product. Panic and anxiety are the most common symptoms. Depersonalization and derealization appear frequently and can be alarming, but they differ from psychosis in that reality testing remains intact throughout.
How long does being too high last?

Duration depends on the route of consumption. Inhaled cannabis typically produces peak effects within 30 minutes, with most acute symptoms resolving within 1 to 3 hours. Edible effects can take 30 minutes to 2 hours to appear, often peak at 2 to 4 hours, and may linger for 6 hours or longer because the liver metabolite 11-hydroxy-THC is more potent and longer-acting than inhaled delta-9-THC.
Why do edibles make people feel more intoxicated than smoking?
After eating cannabis, the liver converts delta-9-THC into 11-hydroxy-THC (11-OH-THC) through first-pass metabolism. This metabolite crosses the blood-brain barrier more efficiently and produces stronger, longer-lasting intoxication. The ratio of 11-OH-THC to delta-9-THC exceeds 1:1 after oral ingestion versus less than 1:20 after inhalation. The delayed onset leads many people to redose before the first dose has fully registered, compounding the effect.
Does CBD help if you’ve taken too much THC?
CBD may modulate THC-induced anxiety at the receptor level. Research suggests CBD can provide relief when baseline anxiety is low and partial relief when it is moderate. Real-world evidence for CBD as an after-the-fact rescue intervention is limited. Most contemporary high-THC cannabis products contain negligible CBD, and consuming a CBD product after the fact has not been studied in controlled human trials for this specific application.
When should you go to the emergency room after consuming too much cannabis?
Seek medical care if you experience chest pain, loss of consciousness, prolonged vomiting, extreme confusion that does not resolve, or any symptom that genuinely frightens you. First-time or pediatric exposures should always be assessed. Cannabinoid hyperemesis syndrome (CHS), associated with chronic heavy use, also requires clinical evaluation. For most adults experiencing an uncomfortable but uncomplicated overconsumption episode, a calm environment, water, and time are appropriate.



Sign up for bi-weekly updates, packed full of cannabis education, recipes, and tips. Your inbox will love it.